
To understand the Coronary Artery Disease (CAD) well, it is important to have basic understanding about anatomy of the heart and how it works. So, let’s begin with it:
ANATOMY OF HEART:
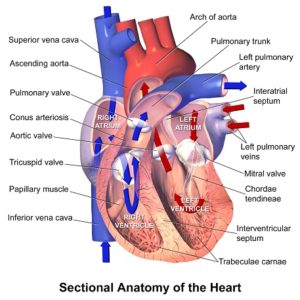
The heart consists of four chambers:
Atria: the two upper chambers (they receive blood).
Ventricles: the two lower chambers (they discharge blood).
The left atria and left ventricle are separated from the right atria and right ventricle by a wall of muscle called the septum.
The wall of the heart consists of three layers of tissue:
Epicardium — protective layer mostly made of connective tissue.
Myocardium — the muscles of the heart.
Endocardium — lines the inside of the heart and protects the valves and chambers.
These layers are covered in a thin protective coating called the pericardium.
How the Heart works:
Right side
The right atrium receives deoxygenated blood from the body through veins called the superior and inferior vena cava (the largest veins in the body).
The right atrium contracts and blood passes to the right ventricle.
Once the right ventricle is full, it contracts and pumps the blood through to the lungs via the pulmonary artery, where it picks up oxygen and offloads carbon dioxide.
Left side
Newly oxygenated blood returns to the left atrium via the pulmonary vein.
The left atrium contracts, pushing blood into the left ventricle.
Once the left ventricle is full, it contracts and pushes the blood back out to the body via the aorta.
Each heartbeat can be split into two parts:
Diastole: the atria and ventricles relax and fill with blood.
Systole: the atria contract (atrial systole) and push blood into the ventricles; then, as the atria start to relax, the ventricles contract (ventricular systole) and pump blood out of the heart.
The Valves
The heart has four valves that help ensure that blood only flows in one direction:
Aortic valve: between the left ventricle and the aorta.
Mitral valve: between the left atrium and the left ventricle.
Pulmonary valve: between the right ventricle and the pulmonary artery.
Tricuspid valve: between the right atrium and right ventricle.
Most people are familiar with the sound of a human heartbeat. It is often described as a “lub-DUB” sound. The “lub” sound is produced by the tricuspid and mitral valves closing, and the “DUB” sound is caused by the closing of the pulmonary and aortic valves.
The heart’s electrical system:
To pump blood throughout the body, the muscles of the heart must be coordinated perfectly — squeezing the blood in the right direction, at the right time, at the right pressure. The heart’s activity is coordinated by electrical impulses.
The electrical signal begins at the sino-atrial (or sinus, SA) node — the heart’s pacemaker, positioned at the top of the right atrium. This signal causes the atria to contract, pushing blood down into the ventricles.
The electrical impulse travels to an area of cells at the bottom of the right atrium called the atrioventricular (AV) node. These cells act as a gate; they slow the signal down so that the atria and ventricles do not contract at the same time — there needs to be a slight delay.
From here, the signal is carried along special fibers called Purkinje fibers within the ventricle walls; they pass the impulse to the heart muscle, causing the ventricles to contract.
Blood vessels:
There are three types of blood vessels:
Arteries: carry oxygenated blood from the heart to the rest of the body. Arteries are strong and stretchy, which helps push blood through the circulatory system. Their elastic walls help keep blood pressure consistent. Arteries branch into smaller arterioles.
Veins: these carry deoxygenated blood back to the heart and increase in size as they get closer to the heart. Veins have thinner walls than arteries.
Capillaries: they connect the smallest arteries to the smallest veins. They have very thin walls, which allow them to exchange compounds with surrounding tissues, such as carbon dioxide, water, oxygen, waste, and nutrients.
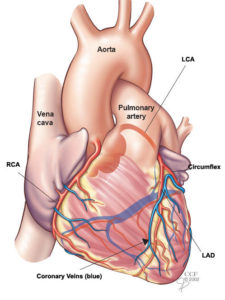
WHAT IS CAD: (CORONARY ARTERY DISEASE) Also known as: CORONARY HEART DISEASE/ ATHEROSCLEROTIC HEART DISEASE
CORONARY ARTERY DISEASE is the narrowing or blockage of the coronary arteries, usually caused by atherosclerosis. Atherosclerosis (sometimes called “hardening” or “clogging” of the arteries) is the build-up of cholesterol and fatty deposits (called plaques) on the inner walls of the arteries. These plaques can restrict blood flow to the heart muscle by physically clogging the artery or by causing abnormal artery tone and function.
Without an adequate blood supply, the heart becomes starved of oxygen and the vital nutrients it needs to work properly. This can cause chest pain called angina. If the blood supply to a portion of the heart muscle is cut off entirely, or if the energy demands of the heart become much greater than its blood supply, a heart attack (injury to the heart muscle) may occur.
CAUSES:
- Smoking
- High blood pressure
- High cholesterol
- Diabetes or insulin resistance
- Sedentary lifestyle
SYMPTOMS:
Chest pain (Angina): Angina is a type of chest pain caused by reduced blood flow to the heart. Angina feels like squeezing, pressure, heaviness, tightness or pain in the chest. It can be sudden or recur over time. Angina is generally triggered by physical or emotional stress.
Shortness of breath: If your heart can’t pump enough blood to meet your body’s needs, you may develop shortness of breath or extreme fatigue with exertion.
Heart Attack (Myocardial Infarction): A completely blocked coronary artery will cause a heart attack. The classic signs and symptoms of a heart attack include crushing pressure in your chest and pain in your shoulder or arm, sometimes with shortness of breath and sweating.
Acute Coronary Syndromes:
Unstable Angina: The angina may occur more frequently, occur more easily at rest, feel more severe, or last longer. Although this can often be relieved with oral medications (such as nitroglycerin), it is unstable and may progress to a heart attack.
Non-ST segment elevation myocardial infarction (NSTEMI): This type of heart attack, or MI, does not cause major changes on an electrocardiogram (ECG). However, chemical markers in the blood indicate that damage has occurred to the heart muscle. In NSTEMI, the blockage may be partial or temporary, so the extent of the damage is usually relatively small.
ST segment elevation myocardial infarction (STEMI): This type of heart attack, or MI, is caused by a sudden blockage in blood supply. It affects a large area of the heart muscle and causes changes on the ECG as well as in blood levels of key chemical markers.
RISK FACTORS:
Non-modifiable risk factors (those that cannot be changed) include:
- Gender. Men have a greater risk of heart attack than women do, and men have heart attacks earlier in life than women. However, beginning at age 70, the risk is equal for men and women.
- Advanced age. Coronary artery disease is more likely to occur as you get older, especially after Age 65.
- Family history of heart disease. You have an increased risk of developing heart disease if you have a parent with a history of heart disease, especially if they were diagnosed before Age 50. Ask your doctor when it’s appropriate for you to start screenings for heart disease so it can be detected and treated early.
- Race. African Americans have more severe high blood pressure than Caucasians and, therefore, have a higher risk of heart disease. The risk of heart disease is also higher among Mexican Americans, American Indians, native Hawaiians, and some Asian Americans. This is partly due to higher rates of obesity and diabetes in these populations.
Modifiable risk factors (those you can treat or control) include:
- Smoking: People who smoke have a significantly increased risk of heart disease. Exposing others to your passive smoke also increases their risk of coronary artery disease
- High blood cholesterol – High levels of cholesterol in your blood can increase the risk of formation of plaque and atherosclerosis. High cholesterol can be caused by a high level of low-density lipoprotein (LDL) cholesterol, known as the “bad” cholesterol. A low level of high-density lipoprotein (HDL) cholesterol, known as the “good” cholesterol, can also contribute to the development of atherosclerosis.
- High blood pressure: Uncontrolled high blood pressure can result in hardening and thickening of your arteries, narrowing the channel through which blood can flow.
- Uncontrolled diabetes– Diabetes is associated with an increased risk of coronary artery disease. Type 2 diabetes and coronary artery disease share similar risk factors, such as obesity and high blood pressure
- Physical inactivity – Lack of exercise also is associated with coronary artery disease and some of its risk factors, as well.
- Overweight or obesity – Excess weight typically worsens other risk factors.
- Stress or anger – Unrelieved stress in your life may damage your arteries as well as worsen other risk factors for coronary artery disease
- Unhealthy Diet– Eating too much food that has high amounts of saturated fat, trans fat, salt and sugar can increase your risk of coronary artery disease.
DIAGNOSIS:
- Asking to you about your medical and family history, check your blood pressure and do a blood test to assess your cholesterol level
- Performing a physical exam
- Performing diagnostic tests
- Electrocardiogram test (ECG) – use the electrocardiogram to evaluate the electrical activity generated by the heart at rest and with activity.
- Laboratory tests – include a number of blood tests used to diagnose and monitor treatment for heart disease
- Minimal invasive testing – such as cardiac catheterization and angiogram, involve inserting catheters into the blood vessels of the heart in order to get a closer look at the coronary arteries
- Nuclear Imaging-produces images by detecting radiation from different parts of the body after the administration of a radioactive tracer material.
- Ultrasound Tests such as echocardiogram use ultrasound, or high frequency sound wave, to create graphic images of the heart’s structures, pumping action, and direction of blood flow.
- Heart scan – Computerized tomography (CT) technologies can help your doctor see calcium deposits in your arteries that can narrow the arteries. If a substantial amount of calcium is discovered, coronary artery disease may be likely.
- Tests used to predict increased risk for coronary artery disease include: C-reactive protein (CRP), complete lipid profile and calcium score screening heart scan.
TREATMENT:
Reducing risk factors and taking medications as prescribed by your Cardiologist. Below are the some of the most advanced and most preferred treatment done by Cardiologists depending upon patients’ condition:
Balloon Angioplasty (PTCA) and stenting (Percutaneous coronary revascularization): These procedures are considered nonsurgical because they are done by a cardiologist (heart doctor), who accesses the heart using a long, thin tube (catheter) that is inserted into a blood vessel, rather than by a surgeon through an incision.
CABG (Coronary Artery Bypass Graft) surgery: One or more blocked coronary arteries are bypassed by a blood vessel graft to restore normal blood flow to the heart. These grafts usually come from the patient’s own arteries and veins located in the chest, arm or leg. The graft goes around the clogged artery (or arteries) to create new pathways for oxygen-rich blood to flow to the heart.
EECP (Enhanced External Counter Pulsation): For patients who have persistent angina symptoms and have exhausted the standard treatments without successful results, EECP may stimulate the openings or formation of small branches of blood vessels (collaterals) to create a natural bypass around narrowed or blocked arteries. EECP is a non-invasive treatment for people, who have chronic, stable angina; who are not receiving adequate relief from angina by taking nitrate medications; and who do not qualify for a procedure such as bypass surgery, angioplasty or stenting.
DISCLAIMER: The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this site. The Site and the Content are provided on an “as is” basis.


